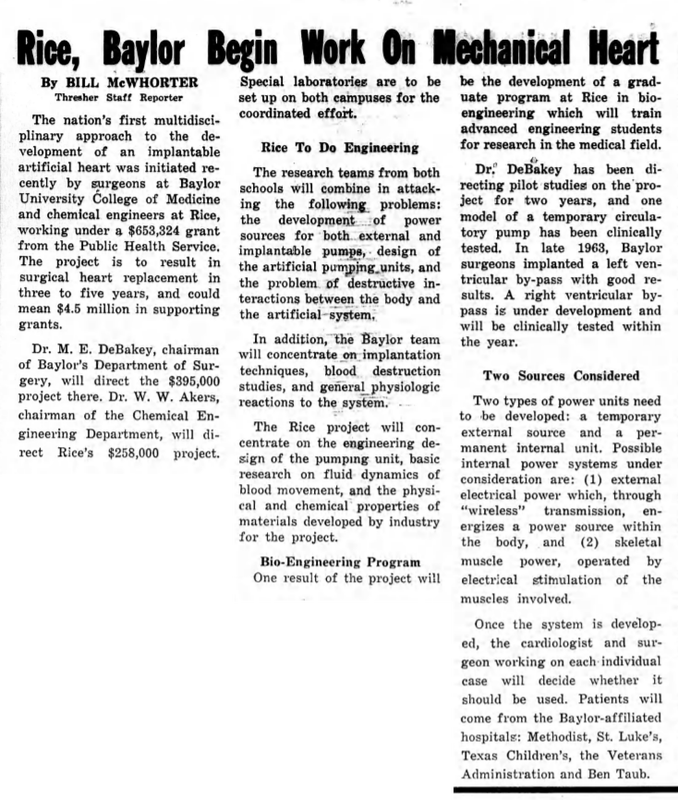
Rice-Baylor CollaborationAn article in The Rice Thresher documents the genesis of the nation's first multidisciplinary approach to the development of an implantable artificial heart, involving surgeons at Baylor College of Medicine and engineers at Rice University.
According to the article, Rice received a $653,324 grant from the U.S. Public Health Service. The U.S. Public Health Service (PHS) is the primary division of the US. Department of Health and Human Services, and includes the FDA, CDC, and NIH. The project's goal was to create a surgical heart replacement in three to five years. |
The Rice Thresher (Houston. Tex.), Vol. 52, No. 3, Ed. 1 Thursday, October 1, 1964
|
breaking barriers
The Rice-Baylor Artificial Heart Program began after Dr. Michael DeBakey, a heart surgeon at the Baylor College of Medicine, approached Rice President Kenneth Pitzer in 1964. Despite progress in treating heart disease, Dr. DeBakey was concerned that there were not enough donors for heart transplants to match the number of patients that needed a new heart.
In 1953, Dr. John Gibbon performed the first successful open-heart surgical procedure with his heart-lung machine, which was developed through 20 years of experimental research. DeBakey’s roller pump, which he had developed as a medical student, was integrated into the heart-lung machine. The heart-lung machine inspired researchers to look into ways that heart function could be replicated through mechanical means.
DeBakey then began researching the development of ventricular assist devices and a total artificial heart. In 1963, DeBakey successfully implanted a ventricular assist device in a patient who required aortic valve replacement. The implant resolved the heart problem, but the patient later passed away due to unrelated reasons.
In the 1950s and early 1960s, there was no major national funding source, such as the NIH or the American Heart Association, for research in the field. In 1963, DeBakey proposed to Senator Lister Hill’s Subcommittee on Health the development of a total artificial heart, asking for funds. This led to the first congressional funding by NIH for research on the artificial heart.
DeBakey realized that the problems in the field were diverse and complex and would require a collaborative multidisciplinary approach. He thus invited researchers from Rice’s Departments of Electronics, Chemistry, Hydraluics, and Engineering to join the program. The new Rice-Baylor Artificial Heart Program received a substantial grant from NIH.
In 1953, Dr. John Gibbon performed the first successful open-heart surgical procedure with his heart-lung machine, which was developed through 20 years of experimental research. DeBakey’s roller pump, which he had developed as a medical student, was integrated into the heart-lung machine. The heart-lung machine inspired researchers to look into ways that heart function could be replicated through mechanical means.
DeBakey then began researching the development of ventricular assist devices and a total artificial heart. In 1963, DeBakey successfully implanted a ventricular assist device in a patient who required aortic valve replacement. The implant resolved the heart problem, but the patient later passed away due to unrelated reasons.
In the 1950s and early 1960s, there was no major national funding source, such as the NIH or the American Heart Association, for research in the field. In 1963, DeBakey proposed to Senator Lister Hill’s Subcommittee on Health the development of a total artificial heart, asking for funds. This led to the first congressional funding by NIH for research on the artificial heart.
DeBakey realized that the problems in the field were diverse and complex and would require a collaborative multidisciplinary approach. He thus invited researchers from Rice’s Departments of Electronics, Chemistry, Hydraluics, and Engineering to join the program. The new Rice-Baylor Artificial Heart Program received a substantial grant from NIH.
Key players
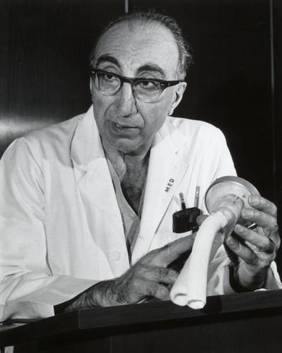
Dr. M. E. DeBakey:
Dr. DeBakey was the chair of Baylor's Department of Surgery. He was the Principal Investigator for the Rice-Baylor Artificial Heart Program. |
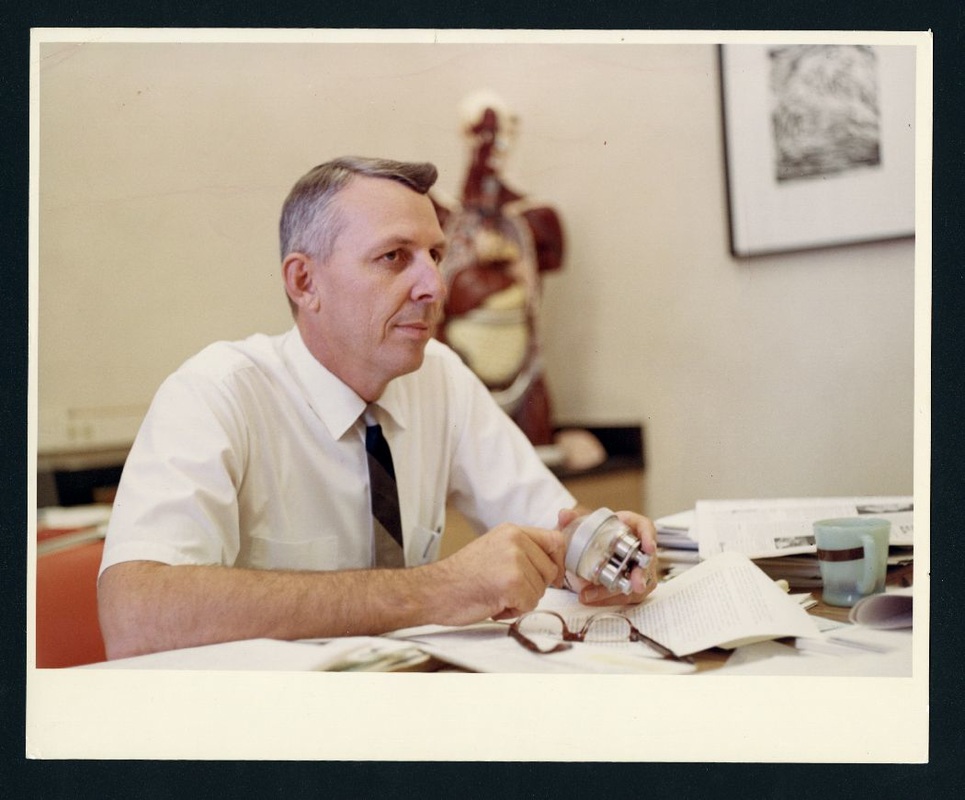
Dr. William W. Akers:
Dr. Akers was the chair of Rice's Chemical Engineering Department from 1955 to 1965. He led the Rice side of the collaboration. |
Multidisciplinary Collaborative approach
|
Collaboration Within Rice
A Rice Thresher article describes the major problems that engineers faced when building the artificial heart. In order to solve these problems, Dr. Akers collaborated with researchers in Rice's mathematical analysis, mechanical engineering, and electrical engineering departments. |

The Rice Thresher (Houston, Tex.), Vol. 53, No. 23, Ed. 1 Thursday, March 31, 1966.
|
|
Collaboration Between Rice and Baylor
Each school tackled different problems. Rice was responsible for researching:
|

Akers manipulating a series of valves on a laboratory rack while conducting research at Baylor College of Medicine.
|
Results
The collaborative effort resulted in the development of a left ventricular assist device (LVAD) that was successfully implanted in animals. The problem of the blood interface was solved through the use of a Dacron velour surface that is compatible with the blood. The LVAD was first successfully used clinically on August 8, 1966, in a 37-year-old woman with heart failure.
The Rice-Baylor collaborative research team also worked on the development of a totally implantable artificial heart. In 1968, they designed a biventricular cardiac prosthesis consisting of two separate units functioning as the right and left ventricles. This total artificial heart model was implanted into calves by a surgical technique similar to transplantation of the human heart. The procedure worked, but the longest survival time was 12.5 hours, and the team concluded that the biventricular pump was feasible, but not ready for human implantation.
The Rice-Baylor collaborative research team also worked on the development of a totally implantable artificial heart. In 1968, they designed a biventricular cardiac prosthesis consisting of two separate units functioning as the right and left ventricles. This total artificial heart model was implanted into calves by a surgical technique similar to transplantation of the human heart. The procedure worked, but the longest survival time was 12.5 hours, and the team concluded that the biventricular pump was feasible, but not ready for human implantation.
future Developments
|
Bio-Medical Engineering Laboratory
The Bio-Medical Engineering Laboratory program was established through funding from the National Heart and Lung Institute. The program was divided into four subgroups: Pumping Systems (mechanical engineering), Bio-materials (biology), Blood and Flow Studies (chemical engineering), and Systems and Instrumentation (electrical engineering). These subgroups collaborated among each other and with Baylor School of Medicine’s Taub Lab for Circulation Assistance Research and U.T. Medical school faculty. The group faced setbacks in “total replacement” due to surgical difficulties and the short-term survival rate of animals with the blood pump implant. Despite these setbacks, faculty praised the multidisciplinary collaborative approach in another Thresher article. Dr. J.W. Clark, who headed the Systems and Instrumentation subgroup in 1974, said the cooperation resulted in “a new perspective on the campus.” Rice faculty tended to focus on basic research, the theoretical side of problems, while Medical Center faculty were directly involved in health care delivery and focused on the more practical side of problems, making clear the clinical implications of engineering advances made at Rice. |
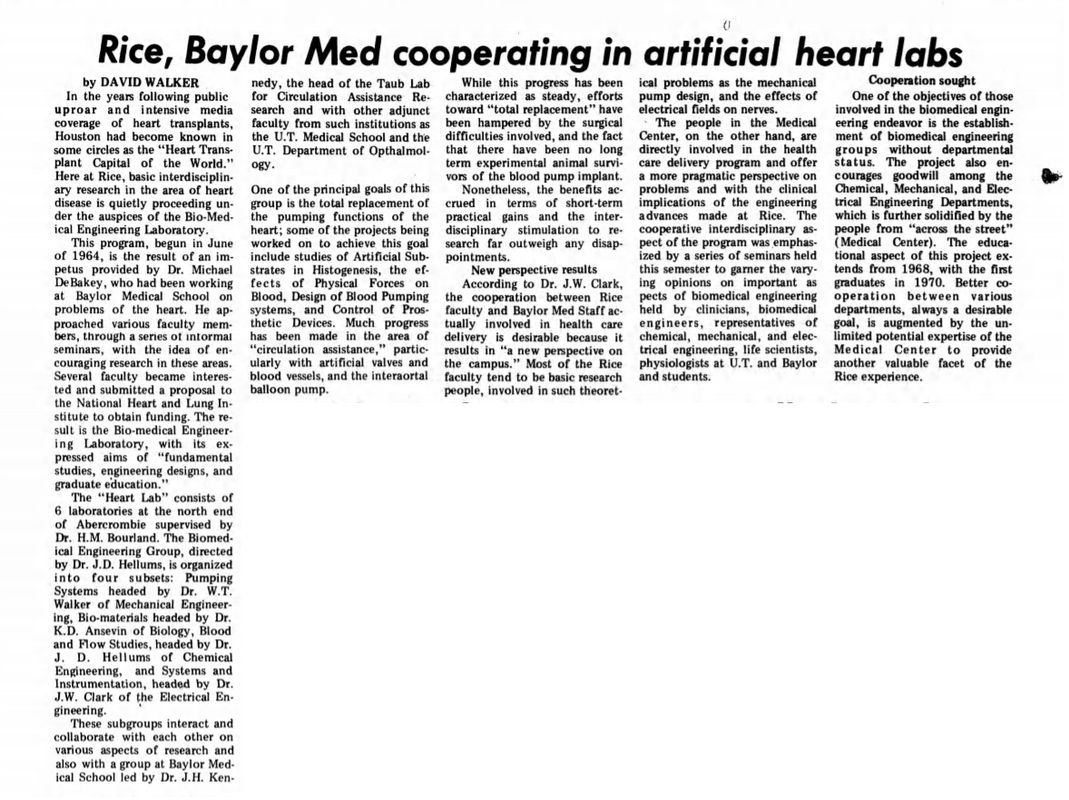
The Rice Thresher (Houston, Tex.), Vol. 62, No. 16, Ed. 1 Thursday, December 5, 1974.
|
Bioscience Research Collaborative
In 2010, the BioScience Research Collaborative (BRC) was founded as “an innovative space where scientists and educators from Rice and other Texas Medical Center (TMC) instituations work together to perform leading research that benefits human medicine and health."
In 2010, the BioScience Research Collaborative (BRC) was founded as “an innovative space where scientists and educators from Rice and other Texas Medical Center (TMC) instituations work together to perform leading research that benefits human medicine and health."
Interinstitutional Agreement
In 2015, Rice and Baylor signed an interinstitutional agreement to facilitate research and teaching collaboration. The agreement states that its purpose is to "facilitate synergies, build structural interfaces and remove barriers to collaboration to leverage the distinctive strengths of each institution." The new agreement is meant to make it easier for faculty, staff, and students from both schools to collaborate by minimizing red tape and paperwork. Read the article here.
In 2015, Rice and Baylor signed an interinstitutional agreement to facilitate research and teaching collaboration. The agreement states that its purpose is to "facilitate synergies, build structural interfaces and remove barriers to collaboration to leverage the distinctive strengths of each institution." The new agreement is meant to make it easier for faculty, staff, and students from both schools to collaborate by minimizing red tape and paperwork. Read the article here.
"Rice and Baylor College of Medicine share a profound commitment to pre-eminence in research, education and service to humanity,"

{kind=link}
{kind=link}